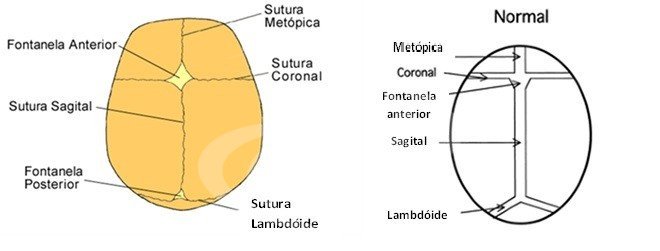
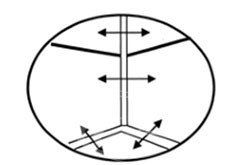
The skull is not made up of a single bone like a helmet, but of bony "plates" that are joined together by lines called sutures. The cranial sutures are there to help shape the head during childbirth and also to shape the growing head. They function as expansion areas that allow the brain to grow inside the skullcap. The sutures normally fuse after the skull has finished growing, however, in some cases they fuse before birth, causing changes to the shape of the head.
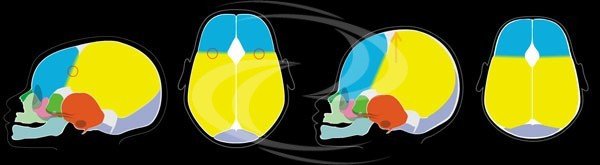
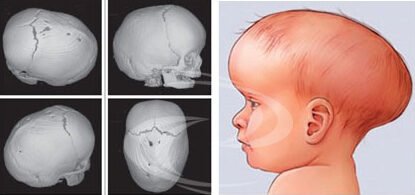
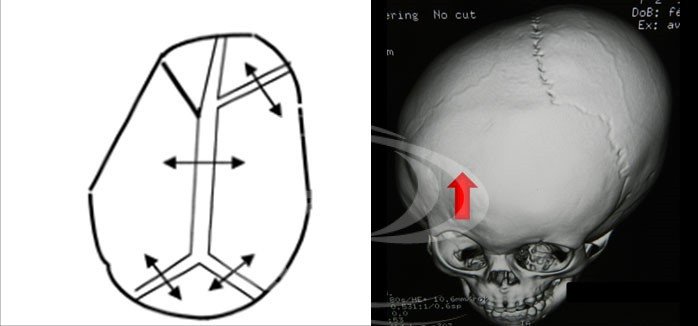
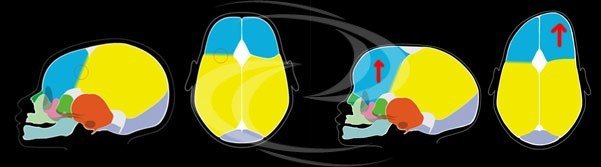
Craniostenosis or craniosynostosis is characterized by the premature fusion of one or more cranial sutures, resulting in deformation of the skull and can be responsible for a growth conflict between the skull and the brain, which sometimes results in chronic intracranial hypertension. This conflict can leave sequelae, notably visual and mental.
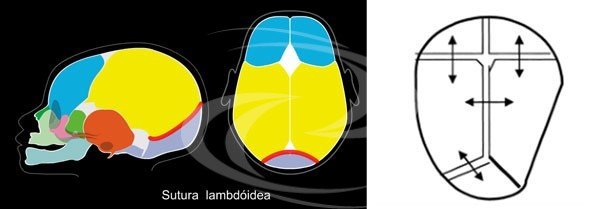
The main cranial sutures are: the sagittal suture, the coronal sutures, the metopic suture and the lambdoid sutures.
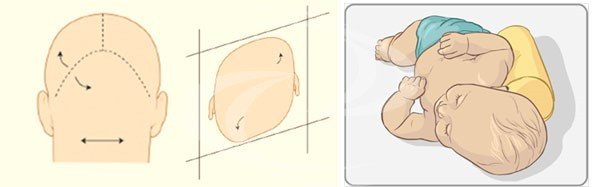
It is important to note that a simple change in the shape of the skull does not characterize craniostenosis. In reality, the main cause of skull deformation is related to external compression forces, often associated with a vicious position of the baby in bed. This alteration is known as positional plagiocephaly, discussed in another section, in which the skull is deformed but the cranial sutures are open.
It is important to note that a simple change in the shape of the skull does not characterize craniostenosis. In reality, the main cause of skull deformation is related to external compression forces, often associated with a vicious position of the baby in bed. This alteration is known as positional plagiocephaly, discussed in another section, in which the skull is deformed but the cranial sutures are open.
 English
English